Most women find out they have an ovarian cyst during a routine ultrasound they almost skipped. The radiologist says something, the report gets handed over, and suddenly there are two words sitting on a page that change everything: ovarian cyst. Next thing you know, you’re drowning in Google searches, bouncing between terrifying possibilities and hopeful reassurances, caught in that exhausting mix of ‘it’s probably nothing’ and deep worry.
The following section provides clear, accurate information on what truly matters regarding ovarian cysts.
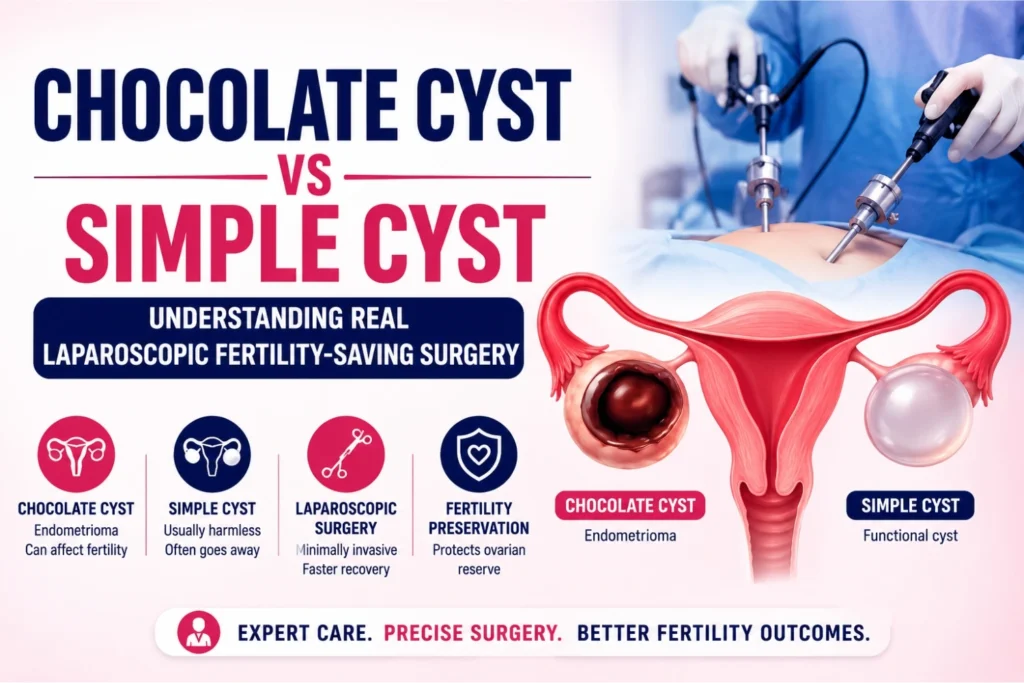
Two Cysts, Two Very Different Problems
Ovarian cysts are not all created equal. Grouping them together is one of the most common sources of confusion for women trying to understand their diagnosis.
What a Simple Cyst Actually Is
A simple cyst is a fluid-filled sac that forms on or within the ovary. In most cases, it develops as part of the normal ovulation process. A follicle grows, releases an egg, and occasionally does not dissolve the way it should. The result is a functional cyst that is usually thin-walled, filled with clear fluid, and in the majority of cases, harmless.
Simple cysts below 5 cm in premenopausal women are often monitored rather than treated immediately. Many resolve on their own within a few menstrual cycles. The lining of a simple cyst is smooth and uncomplicated, which matters a great deal when surgery eventually becomes necessary, because removing it cleanly and preserving the surrounding ovarian tissue is far more straightforward.
What a Chocolate Cyst Is and Why It Is Different
A chocolate cyst is something else entirely. The clinical name is endometrioma, and it forms when endometrial tissue, the tissue that normally lines the inside of the uterus, grows on or inside the ovary. Every month, this tissue behaves exactly the way the uterine lining does: it responds to hormonal cycles, breaks down, and bleeds. Except there is nowhere for that blood to go. Over time, it accumulates inside the cyst, oxidizes, and turns into a thick, dark brown fluid. That is where the name comes from.
The contents look like old chocolate. The implications for fertility are far less sweet. Endometriomas are directly associated with reduced ovarian reserve. The inflammatory environment they create damages the healthy follicles surrounding them. Women with chocolate cysts often have lower AMH levels, fewer eggs available for ovulation, and a higher likelihood of adhesions that distort the normal anatomy of the pelvis. Left untreated, they can silently compromise fertility over months and years.
When Surgery Becomes the Answer
Not every ovarian cyst requires surgery. The decision depends on the size of the cyst, the type, the symptoms, and what the woman’s fertility goals look like.
Signs That Surgery Cannot Wait
Severe pelvic pain that disrupts daily life, cysts that continue to grow despite watchful waiting, suspicion of malignancy based on imaging characteristics, or cysts that are large enough to risk torsion (the ovary twisting on itself, cutting off its blood supply) all point toward surgical intervention.
For chocolate cysts specifically, the threshold for surgery is also tied to fertility planning. A woman who is trying to conceive and has a significant endometrioma is not in a position to simply wait and watch. The cyst is actively working against ovarian function with every passing month.
Laparoscopic Surgery
Laparoscopic surgery is the gold standard for managing ovarian cysts, and the reason is straightforward. Smaller incisions, faster recovery, less trauma to surrounding tissue, and far better visualization than open surgery can offer.
How the Procedure Works Step by Step
The surgeon makes two to three small incisions in the abdomen. A laparoscope, a thin camera, is inserted through one incision to give a real-time view of the internal anatomy on a monitor. Surgical instruments enter through the remaining incisions.
Carbon dioxide gas is used to inflate the abdominal cavity, creating space to work without the instruments pressing against organs. Once the ovary is clearly visible, the surgical approach changes depending on what type of cyst is being removed.
Removing a Simple Cyst
With a simple cyst, the wall is thin and the fluid inside is clear. The surgeon carefully opens the cyst, drains the fluid, and then excises the cyst wall completely. The key word is completely. Leaving any cyst wall tissue behind dramatically increases the rate of recurrence. Once the wall is removed, the ovary is inspected, any bleeding points are addressed, and the remaining ovarian tissue is preserved.
Removing a Chocolate Cyst
A chocolate cyst demands considerably more precision. The cyst wall in an endometrioma is often adherent to the surrounding ovarian tissue, which means it does not peel away cleanly. Surgeons must carefully dissect the cyst away from the healthy cortex of the ovary without destroying the follicles embedded in that cortex.
The thick, dark contents of the cyst are drained, the cavity is thoroughly irrigated, and then the painstaking work of separating the cyst wall from the ovarian tissue begins. This is where surgical experience makes the real difference. Aggressive removal that strips too much ovarian tissue can leave a woman with significantly reduced ovarian reserve post-surgery. Incomplete removal leads to recurrence. The goal is to remove the entire cyst wall while protecting every viable follicle in the ovary.
Dr. Sophia Umair Bajwa covers this surgical process in real-time on her YouTube channel, with actual operative footage from the operation theatre. Watching a step-by-step walkthrough of how these cysts are approached under laparoscopy gives a level of clarity that no diagram or description can fully replicate. Her channel is genuinely worth a visit for anyone trying to understand what this surgery looks like in practice.
Why Preserving the Ovary Is the Priority
There was a time when the standard response to a large or problematic ovarian cyst was simply to remove the entire ovary. That approach has largely been abandoned in the context of reproductive-age women, and for good reason.
The ovary is not just a structure. It is a woman’s egg reserve. Removing one ovary can reduce the available follicle pool, and in women who already have reduced ovarian reserve due to an endometrioma, losing an ovary compounds the problem significantly.
Fertility-preserving laparoscopic surgery focuses on cystectomy, removing only the cyst while keeping the ovary intact. Even in complex cases involving dense adhesions or bilateral cysts (cysts on both ovaries), the surgical goal remains the same: remove the pathology, protect the function.
After Surgery: What to Do
Recovery from laparoscopic cystectomy is typically faster than patients anticipate. Most women are discharged within 24 hours. Full recovery takes one to two weeks for most, with a return to normal activity following shortly after.
For women with endometriomas, surgery addresses the immediate mechanical problem. Recurrence, however, is a real consideration, with rates reported between 15 and 30 percent within five years if underlying endometriosis is not managed medically after surgery.
Hormonal therapy post-surgery is often recommended to suppress the conditions that allow endometrial tissue to grow. Fertility treatment, if needed, is typically initiated a few months after surgical recovery.
Family Fertility & IVF Center in Lahore takes a fertility-focused approach to ovarian cyst diagnosis and treatment from the very first consultation. The center handles everything from initial assessment and imaging interpretation to surgical intervention and post-operative fertility planning. For anyone in Pakistan looking for the best IVF center in Lahore, this is the kind of medical approach that changes outcomes.
Choosing the Right Surgical Team
Laparoscopic cystectomy sounds simple on paper. In practice, the outcome depends heavily on the skill and experience of the surgeon performing it. Incomplete cyst wall removal, damage to healthy ovarian tissue, or missed adhesions can all have consequences that outlast the surgery itself.
Dr. Sophia Umair Bajwa and the surgical team at Family Fertility & IVF Center bring both clinical precision and a fertility-first mindset to every procedure. That combination matters more than most patients realize at the beginning of treatment.
If anything in this guide raised questions, leave a comment on the YouTube video and the team will address it. There is no shortage of topics to unpack, and every question helps shape what gets covered next.