You get an ultrasound. The report comes back with “ovarian cyst.” And before you have even spoken to your doctor properly, someone has already suggested surgery.
That is where things go wrong for a lot of women. Not because surgery is always the wrong answer, but because agreeing to it without understanding what type of cyst you have, what it is actually doing, and what the surgical risks are to your ovarian reserve, can cost you fertility you did not even know you were losing.
Ovarian cysts are not all the same. The type determines the risk. The type determines whether surgery is even necessary. And critically, the type determines how urgently your fertility needs to be factored into the treatment decision.
What Ovarian Cysts Are
An ovarian cyst is a fluid-filled sac that develops on or inside the ovary. Most women will have one at some point in their lives. Many resolve on their own without any intervention. The problem is that “ovarian cyst” gets used as a blanket term for conditions that are clinically very different from each other.
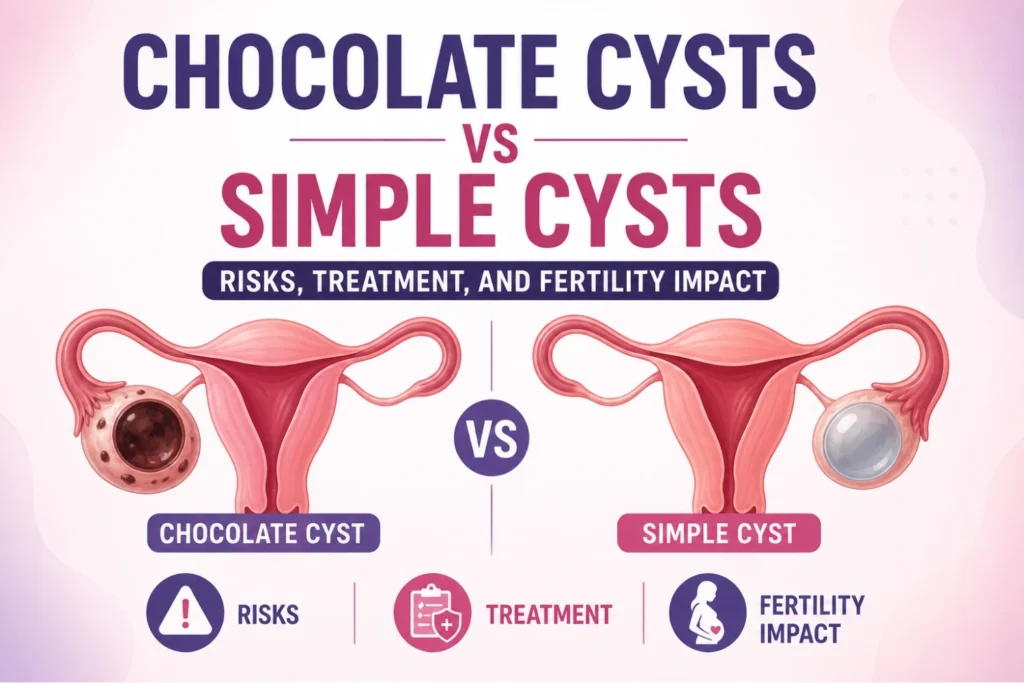
The two types that come up most in fertility discussions are simple cysts and chocolate cysts, and confusing the two leads to very different treatment mistakes.
Simple Cysts: Usually Not the Emergency They Sound Like
Simple cysts are exactly what the name suggests. They are thin-walled, fluid-filled, and show up on ultrasound with a clean, straightforward appearance. Most of them are functional cysts, meaning they developed as part of a normal ovulation cycle and simply did not resolve the way they should have.
A follicle that did not release its egg becomes a follicular cyst. A corpus luteum that did not break down becomes a corpus luteum cyst. Both are common. Both are usually temporary.
When Simple Cysts Need Attention
A simple cyst under 5 to 6 centimeters in a woman of reproductive age is almost always managed with watchful waiting. A repeat ultrasound after one or two menstrual cycles will typically show it has shrunk or disappeared entirely.
Surgery for a simple cyst that is small, asymptomatic, and showing no suspicious features on imaging is often unnecessary. Rushing into an operation for a cyst that would have resolved on its own is a real phenomenon, and it carries real risks to the ovary.
When a simple cyst is large, causing significant pain, showing growth on repeat imaging, or has features that raise concern, the conversation about intervention becomes appropriate. But the starting point should always be proper assessment, not a reflexive surgical referral.
Chocolate Cysts: A Completely Different Problem
A chocolate cyst, medically called an endometrioma, is a type of ovarian cyst caused by endometriosis. When endometrial tissue grows outside the uterus and attaches to the ovary, it forms a cyst that fills with old menstrual blood. That blood breaks down over time into a thick, dark, tar-like fluid. The color is where the name comes from.
Endometriomas do not behave like functional cysts. They do not resolve on their own. They tend to grow. They cause inflammation around the ovary. And they are directly associated with reduced ovarian reserve, even before any surgical intervention.
How Chocolate Cysts Damage Fertility
This is the part that does not get explained clearly enough. An endometrioma sitting on the ovary is not just occupying space. The inflammatory environment it creates actively damages the surrounding ovarian tissue, which contains the primordial follicles that make up a woman’s egg reserve.
Studies consistently show that women with endometriomas have lower AMH (anti-Mullerian hormone) levels compared to women without them, indicating reduced ovarian reserve. The damage is ongoing for as long as the cyst is present.
The cruel irony is that surgery to remove the cyst can also reduce AMH. Because endometriomas are embedded in ovarian tissue, removing them without inadvertently taking healthy follicle-containing tissue along with them requires a level of surgical precision that not every surgeon applies.
The Surgery Question: When Is It Worth It?
This is where the decision becomes genuinely nuanced and where the wrong advice causes the most harm.
Dr. Sophia Umair Bajwa is clear on this point: surgery for an endometrioma is not automatically the right answer just because the cyst exists. The decision depends on the size, the symptoms, the patient’s current AMH and antral follicle count, and whether she is planning to pursue IVF.
When Surgery Makes Sense
An endometrioma over 4 centimeters that is causing significant pelvic pain. A cyst that is growing on serial imaging. Diagnostic uncertainty about the cyst’s nature. A situation where the cyst is physically compromising egg retrieval access during an IVF cycle. These are the scenarios where surgical intervention has a genuine clinical rationale.
When Proceeding Directly to IVF Makes More Sense
For a woman with a known endometrioma, already reduced ovarian reserve, and a clear fertility goal, operating on the cyst before IVF may do more harm than good. Removing the cyst risks further reducing the egg reserve. In this scenario, many fertility specialists recommend proceeding directly to IVF, retrieving as many eggs as possible from the current reserve, and managing the endometrioma medically rather than surgically.
This is not a fringe opinion. It is a position supported by reproductive medicine guidelines and by the clinical experience of specialists who have seen what post-surgical AMH drops look like in women who could not afford to lose that reserve.
Why Laparoscopy Is the Only Acceptable Surgical Approach
If surgery is decided upon, the technique matters enormously. Open surgery for an ovarian cyst in a woman who wants to preserve fertility is not the standard of care. Laparoscopy is.
Laparoscopic cyst removal uses small keyhole incisions, a camera, and specialized instruments. The surgeon has direct magnified visualization of the ovary. The cyst wall is carefully separated from the surrounding ovarian tissue. When done correctly by a surgeon experienced in fertility-preserving technique, the damage to the ovarian cortex is minimized.
The key phrase there is “when done correctly.” Laparoscopy in inexperienced hands still carries the same risk of inadvertent ovarian tissue removal. The approach reduces risk. The surgeon’s skill and commitment to preserving ovarian tissue determines the outcome.
Get the Right Assessment Before You Decide
Before any cyst becomes a surgical decision, a complete picture is needed. Ultrasound with detailed cyst characterization. AMH and antral follicle count to establish baseline ovarian reserve. A clear understanding of symptoms and their impact. And a frank conversation about fertility goals.
On her YouTube channel, Dr. Sophia Umair Bajwa walks you through actual surgical cases, showing how chocolate cysts and simple cysts are handled in the operation theatre. If watching real procedures helps you make better-informed choices, you’ll find her channel really helpful.
At Family Fertility & IVF Center in Lahore, ovarian cyst cases are assessed with fertility preservation at the center of every treatment decision. The question is never just “should this cyst come out.” The question is what the best outcome looks like for that specific woman’s fertility. For anyone dealing with an ovarian cyst diagnosis in Lahore and trying to understand what it actually means for their reproductive future, Family Fertility & IVF Center is where that conversation belongs.
Got a question about ovarian cysts, endometriosis, or fertility that deserves a proper answer? Drop it in the comments below or on the YouTube video. If it is something more women need to hear, it becomes the next piece of content.